Thanks for joining this month’s episode of BlisterPrevention Office Hours. We have received heaps of really great questions this month, and unfortunately, I’m not going to be able to get to them all. In fact, my plan in, instead of giving them lip service, I’m going to cover these and more in next month’s Office Hours. But if anyone has asked a question and they’re on the call, just let me know and I’ll be sure to answer that question, because I don’t want to let anyone down if I’ve gone to the effort of joining live. But if you are watching the replay of this, I’m going to do a full Q&A in December. So the first Wednesday in December will be pure Q&A, including the great questions that were posed this month.
Today we’re going to talk about hydrocolloids.
What are they? They’re a category of wound dressing. Now, I’ve underlined “wound” because this becomes important a little bit later. But essentially they need an exudative wound base to be able to interact with to work their magic. So they contain hydrophilic particles that absorb moisture from the wound (on the underside of the dressing), and they’re bound to a hydrophobic polymer that keeps the external environment out. They have two use cases; that is ulcer dressings and blister dressings. And we’re going to have a look at both of these use cases.
So let’s make a start with the ulcer dressings.
I think it’s fair to say that the most common ones are Duoderm and Comfeel, at least from my perspective. Duoderm is very familiar, we’ve been using it for years and also Comfeel – I used to have Comfeel in my blister kits until I got my own brand. So I’m familiar with that one, too.
What types of wounds were they good for? Lightly exudating non-infected lesions. So, shallow ulcers, superficial abrasions, deroofed blisters and minor burns was mentioned as well. These are the types of wounds.
As podiatrists, what do we require in a hydrocolloid ulcer dressing? Hydrocolloids for podiatrists need it to be sterile. We needed to be individually packaged so that when we open one, we’re not opening the whole lot. We also know that we need to anchor the edges with fixation tape. And we also know that ideally, dressings stay on for as long as possible, maybe up to a week. Certainly with hydrocolloids, more than 24 hours. So it’s important to match the ulcer dressing to the lesion so that you’re not having to change it too frequently. And of course it needs to be registered with the relevant health authorities.
What’s not ideal about hydrocolloid ulcer dressings? Most of them are too big for the types of lesions we want to put them on, or that we often see. The most common dressing size is the 10cm by 10cm. But we want to put them on relatively small lesions (shallow ulcers and deroofed blisters). These lesions usually present on these areas of the foot. And yet if we open a 10cm by 10cm, it is just far too much there and one of three things happen. Either:
- We open it use it a little bit and then fold it back down as best we can to keep it clean, but it’s unsterile. We’re probably using them on multiple patients and there’s a real cross infection risk.
- Or we use a little bit and throw the rest out, which seems a bit of a waste.
- Or we just don’t use them, even when they’re clinically indicated because it’s just not cost effective to do so.
I had a look at a few Podiatry Suppliers for some search terms to see what’s available. These are just the Podiatry Suppliers that I know – there may be some that I’ve missed, I’m sorry about that.
“Duoderm”
In searching for duoderm. There’s mainly the 10cm by 10cm size. I didn’t even know there was a 7.5cm x 7.5cm size that Algeos has.
It’s worth mentioning that Duoderm has this nice little one called a Duoderm Spot. I think it’s a Duoderm Extra Thin Spot. None of the Podiatry Suppliers have this, but it’s a great little size for a small ulcer or deroofed blister say under one or two met heads or in the arch or even at the back of the heel. I got mine from Independence Australia, if you want to look for them. And the fixation tape is just something that I cut out. So the Duoderm Spots are a good one.
“Comfeel”
I looked for Comfeel and to my surprise it just wasn’t available at the Podiatry Suppliers that I know of, which is unexpected because as I said, I used to put that in my blister kits.
“Hydroactive”
Hydroactive is a term that is often used synonymously with hydrocolloid. They’re a bit different. The brands here the Biotain and the Allevyn. They’re more like a foam dressing rather than a typical hydrocolloid dressing. They are, to my understanding, for wounds that are a bit more exudative. So they absorb a bit more exudate than hydrocolloids do. But they’re getting into some small sizes.
“Hydrocolloid”
And hydrocolloid, we’ve got the 10cm by 10cm, the 7.5cm x 7.5cm. Footmedics has a brand I wasn’t aware of called ActiveHeal in 5cm x 7.5cm. And Briggate Medical has our BlisterPod range. So we’re getting into these more Compeed-type sizes that are nice little sizes and shapes for these lesions that we are often presented with.
BlisterPod
I’m going to introduce you to our new hydrocolloid range called BlisterPod hydrocolloids. They’re blister dressings, but they’re hydrocoloids so they can be used on all of thoserelevant types of lesions. And this is what they look like. So these are the relative sizes and actual pictures of them in place. They’re very similar to Compeed sizes and shapes and that’s what makes them so convenient.
Type of skin more likely to deroof (plantar skin versus thinner less thethered skin)
When you think about what types of lesions that are more likely to deroof in terms of blisters, it’s the type of skin that is thinner and less tethered to underlying structures. So that is basically skin on the dorsum and the posterior heel, as opposed to plantar skin. When they were doing experimental blister research, I think it was Sulzberger back in the 1960s, they commented about this. They were producing blisters on the forearm or the shin or something and they were noticing that it never actually got to the blister stage. As in, it never became fluid-filled or it wasn’t fluid-filled for long. Because we know it takes up to two hours for a blister to fully fill with fluid. But the roof was shearing off before that happened. And so our patients are often coming in with “rubs” or scrapes or abrasions where the initial injury was probably the intra-epidermal tear of the blister, but they never actually saw the blister.
It’s these smaller areas that we want to be able to put hydrocolloids on because they’re going to respond really well to hydrocolloids. But when we open up an ulcer dressing that’s by 10cm square, it just really seems a bit of a waste. The size and the shape matters! They’re convenient. We can use them in a hygienic way. And they’re just easy to apply.
So that’s ulcer dressings.
We’re going to have a look at the blister scenario now.
This is the use case that I’m more involved in. The three main brands are:
- Compeed is the most well-known brand by far.
- Band-Aid has their own brand called advanced healing.
- And we have our BlisterPod brand.
What blisters should hydrocolloids be used on? Remember I said they’re a category of wound dressing. So they really should only be used on deroofed blisters – where there’s a raw blister base that’s weeping that the hydrocolloid particles can interact with.
But the thing is, they’re being used on every blister situation, from blister prevention to intact and torn blisters. And the problem there is, they’re very adhesive to dry skin. If you do have a blister there already or you put one on as prevention and it doesn’t work and you get a blister underneath it, when you go to remove that hydrocolloid, it’s very common that the hydrocolloid will peel the whole blister roof off with it. This is a really common scenario in active situations. Maybe not in relatively sedentary situations, but definitely in long distance hiking and running, it’s a big thing!
However, if we have patients that are relatively sedentary, it’s fair enough to expect Compeed to provide some prevention power. The way they can possibly work is:
- They cushion, so they reduce pressure a little bit.
- And they spread shear load, which is what adhesive products like moleskin and tape do.
It’s important to understand, adhesive products don’t negate shear load. They just spread it over a bit of a larger area, thereby reducing peak shear at a particular location. It’s easy to think that if we adhere something to the skin it is going to 100% prevent blisters. But that is using the mindset or the paradigm of blister-causation being rubbing. Remember, blisters aren’t caused by rubbing on the skin surface.
Hydrocolloid blister dressings are often used incorrectly and that’s very frequently leading to worsening blister situations. To the point where some races discourage them and even ban them. In some ultramarathons, they have to have their kit checked and they have to have certain stuff in there and they’re not allowed to have certain stuff in there. The reason that race medics don’t want people having Compeed or hydrocolloids is because runners are using them in the wrong situation. But part of that isn’t the runners’ fault – it’s often the instructions-for-use on the packaging. They’re really less than ideal, and we’re going to go through that in a moment.
Hydrocolloid rollback
It’s very common that hydrocolloids without fixation get that little bit of rollback. And when they stick to a sock, they really meld into the sock. It’s just such a difficult situation to pick it out of the sock, and race medics are having to troubleshoot these situations. So that’s partly what’s going on there.
People are making other mistakes too.
Anchoring
They don’t realise that the anchoring is important because they’re not told – the instructions-for-use don’t make any mention of it. But it’s very easy to get hydrocolloid rollback – very, very easy. This is an ultra marathon situation where this person made two mistakes. Number one, they put a Compeed on a hotspot expecting it to prevent the blister. They got a blister anyway (not enough blister prevention power). But the second mistake they made was there was no fixation. And so they suffered a bit of rollback, it stuck to glue to the sock, they peeled their sock off and it peeled the whole blister roof off. The difficult thing here is not only have we sustained a worsening blister situation, but this person now needs a hydrocolloid for their deroofed blister. But now they think hydrocolloids are the root of all evil. This is why hydrocolloids have a really bad rap, because of these poor instructions-for-use, and this over-inflated expectation about how much power they have to prevent blisters. People will either love them or hate them and this is the reason they hate them.
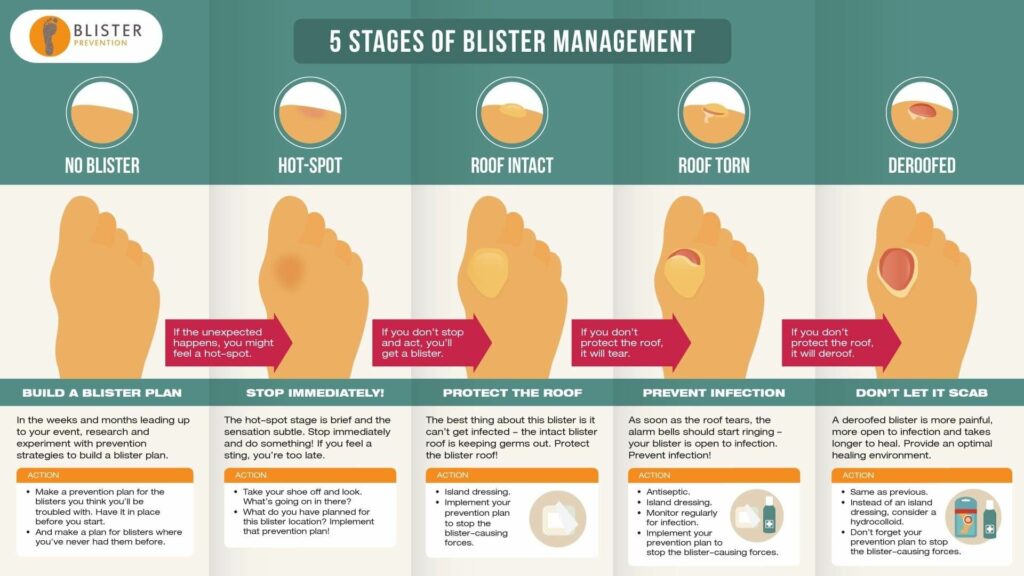
Leave it on for at least 24 hours (if not longer)
People don’t know that it’s ideal to leave a dressing on for as long as possible, up to week. So that expectation needs to be set in the instructions-for-use.
Hydrocolloid white gel bubble
They don’t know what this white gel bubble is. You and I know that this is just a sign that the blister fluids are combining with the hydrocolloid particles, and this is a normal situation. But people jump to the conclusion that their blister is infected. I get lots of emails and comments about this and they’re freaking out thinking that things have got worse than they don’t know what to do next.
Anxiety at dressing changes
There’s also anxiety at addressing changes because you take it off and it’s gooey and it smells bad. Again, we know this is a normal presentation, but people are jumping to the conclusion that this hydrocolloid has caused their blister to become infected. So we need to set expectations there.
First aid, not cure-all
And we also need to set expectations about exactly what we can expect from a hydrocolloid. How does it work? Hydrocolloids are literally first aid. They’re like Betadine and a Band-Aid. So, Betadine and a Band-Aid, or Betadine and a hydrocolloid, that’s first aid for a blister. It’s the bare minimum that needs to be done. But what it doesn’t do is it doesn’t reduce the blister-causing forces well enough to guarantee that that blister will feel better (less painful) when we put our shoe back on and keep walking or running. And also stop that blister from getting worse. So, we’ve got to implement a really good prevention as well as the first aid, and that’s what’s classified as really meaningful blister treatment. This becomes really important when you’re doing foot care at athletic events.
What our patients should be looking for in a hydrocolloid
The requirements that our patients should be looking for in a hydrocolloid, which they really don’t have any idea about is:
- They don’t realise they should be sterile and individually-wrapped. Because these are going on open wounds. Compeed provides this little plastic container, which is nice. But if you take one of these out and put it in your handbag, one in your gym bag, one in your desk at work, one in the medicine cabinet at home, you’ll realise that the edges pick up bits of grass and hair and goodness knows what. It’s not the kind of thing you want to be putting on an open wound.
- They need to be individually-wrapped so that they can remain sterile until the time comes to use it.
- And I’ve got a bit of a bee in my bonnet about instructions-for-use, because this is where most of the other brands fall down. Compeed encourage the use of their product on any blister, including as a blister prevention. That is literally responsible for why there’s a lot of negative talk about hydrocolloids, and worsening blister situations. Band-Aid actively discourages the use of an antiseptic. And the reason they do that is customers are complaining that it doesn’t stay on for long enough. So they discourage the use of an antiseptic. But hydrocolloids are occlusive and they should be used on non-infected wounds. I don’t think there’s many blisters that would deroof in a clean environment. They’re generally deroofing in the shoe and there will be colonization there for sure. So it’s really not a great idea to discourage people to use antiseptic.
- The better idea would be to lock those edges in – anchor them with some fixation tape that’s going to prevent the rollback. It’s going to prolong the length of time that dressing will stay on. And the edges aren’t going to lift. So it’s going to keep the blister clean.
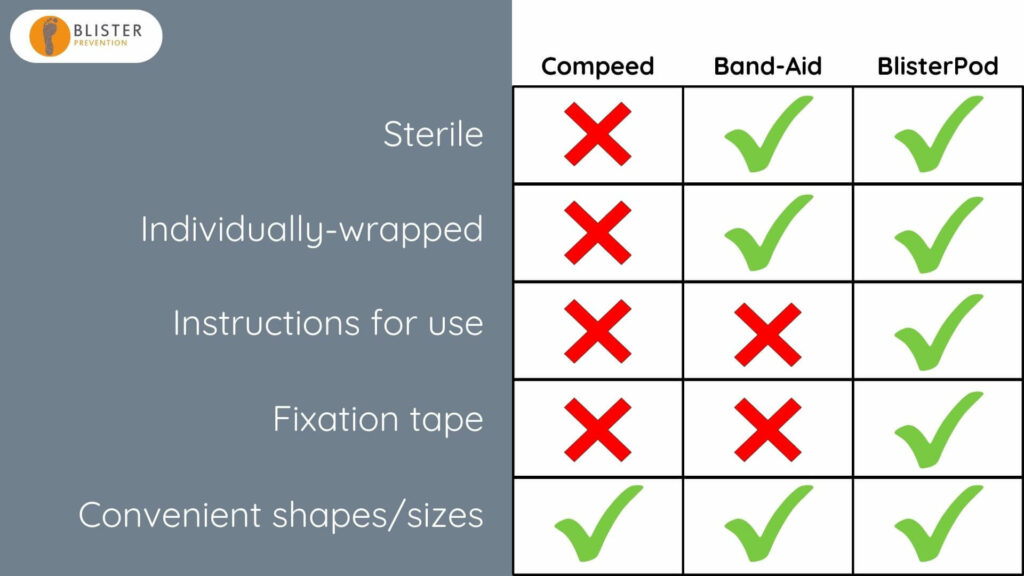
Pros and cons of hydrocolloid blister plasters
So looking at the pros and cons at these three brands that we’ve looked at. Compeed is great in that they have these convenient shapes and sizes – that’s a big plus, for sure. Band-Aid goes a step further by having them sterile and individually-wrapped, which is sensational. But our BlisterPod brand is the only brand that ticks all the boxes. We’ve put a lot of effort into this because it’s a real pain-point for people. It’s plain to see we need really good instructions for use and the fixation tape – not just mentioning that we need it, but we’re actually providing it with the product.
Our brand new hydrocolloids come in four pack arrangements:
- LARGE 6-Pack
- MEDIUM 6-Pack
- SMALL 6-Pack
- MIXED 6-Packs
Let’s watch this 90 sec video where I show you what they look like in the flesh.
- We’ve got the instructions for use on the back of the packet.
- But we’ve also got this extended blister treatment insert that is in five languages.
- We’ve got the six sterile and individually wrapped hydrocolloids.
- And we have the six fixation tapes.
Podiatrist are…
Okay in conclusion, podiatrist are:
- Using a small piece of a hydrocolloid and keeping the rest in an unsterile way, risking cross infection.
- Or they’re wasting unused product.
- Or they’re just not using hydrocolloids in the first place, even when they’re clinically indicated because it’s not cost-effective to do so.
The general public is…
The general public is:
- unwittingly using them for the wrong blister situations, thanks to some dubious instructions-for-use.
- They’re using non-sterile hydrocolloids because the main brand provides them non-sterile.
- They’re not using antiseptic because of some dubious instructions for use.
- They’re not anchoring the edges because they don’t even know to, and they’re certainly not told to.
- They’re anxious at dressing changes because they just don’t know what to expect, or what normal looks like.
- And they’re not implementing further prevention because they have an inflated expectation about the prevention power of hydrocolloids. Remember, they only provide a little bit of blister prevention power (they cushion a little bit, and they spread shear load a little bit) but that’s often not enough in an athletic situation.
BlisterPod Hydrocolloid Blister Dressings
The BlisterPod range of hydrocolloids are the only hydrocolloids in:
- the convenient shapes and sizes of Compeed
- they’re sterile and individually packaged
- they include the fixation tape
- they have great instructions that really set our patients and our customers up for good blister outcomes
- and they’re registered with the TGA
Here are a couple of photos to show you exactly what you get in each pack. They retail for between $9.95 and $16.95.
- You can get them from our website blister-prevention.com. You can buy them retail yourself or at least if you feel like it’s something that your patients would benefit from you can point them in that direction.
- You can also get them at Briggate Medical.
- And you can get them from us at wholesale rates.
If you’re a wholesale partner of ours, then you already have access to these. If not, fill out the application on our wholesale page here if you’d like to offer blister products for your practice and we’ll get you access to those wholesale rates.
You can purchase our hydrocolloids wholesale as individual six packs, and you can also purchase them as cartons. There are ten 6-packs in each carton. The good thing about the carton is, apart from further savings, is we’ve got a tear away for you to sit them on a retail shelf or reception desk. But of course, you can hang them in your retail space too.

Q&A
As I mentioned at the start, we don’t have time for Q&A today, I’m going to do a full Q&A session during the next episode. But Emily, you asked the question when you registered and I want to get to that seeing as though you made the effort to join live.
Emily asked:
What’s the best blister prevention for kids with new school shoes, even when fitted correctly?
It depends where the blister is. There’s not a single answer for this question, because we need to really think about where the blister is. Now, from my experience, the most common blister in school shoes is the blister on the back of the heel.
The best prevention, in my opinion, is easily the ENGO Patches. They’re the most convenient and the long-lasting. However, school kids have a habit of forcing their heel into the shoe, often without undoing their laces. ENGO Patches can be dislodged when you do this, especially in the early stages of application. As you force your heel down, the sock catches the top of the patch, and bit by bit more of that patch will be revealed. It’ll collect sock fluff and after a while it won’t be very stuck on. So that’s a bit of a downside for school kids and ENGO Heel Patches. They need to take a bit of care and guide their heel over the top of the patch
Other than that, thick padded socks can help a lot. Lacing techniques to really keep that heel locked in. This is tricky with school shoes because school shoes typically don’t have enough eyelets. I had a school shoe the other day with only three pairs of eyelets! Calf stretches are an important thing to get started on. They’re not going to have an immediate effect, but with blister-causing shear being generated first of all from bone movement relative to skin movement, a tight calf is pulling on the posterior heel sooner and there’s more force lifting that heel bone up and that leads to more blister-causing shear. And lastly, tape will help a bit. For some it will be enough to keep them blister-free. But if not, don’t be surprised, just move on to something that works better at reducing the magnitude of shear deformation (bone and skin moving out of synch).
👋