There’s a lot of confusion around the aim of blister treatment in terms of the blister roof integrity. Some races, for example, Marathon des Sables routinely roof blisters. Yet most medical advice recommends against lancing – to keep the blister intact. Myself, in race support situations, I usually lance. Yet in my clinic, I have a more even spread of deroofing, lancing and leaving intact. So, understandably, there’s a lot of confusion around this issue. Should blisters should be lanced, deroofed or left alone? Let’s look at the clinical nuances of this topic.
Five blister stages
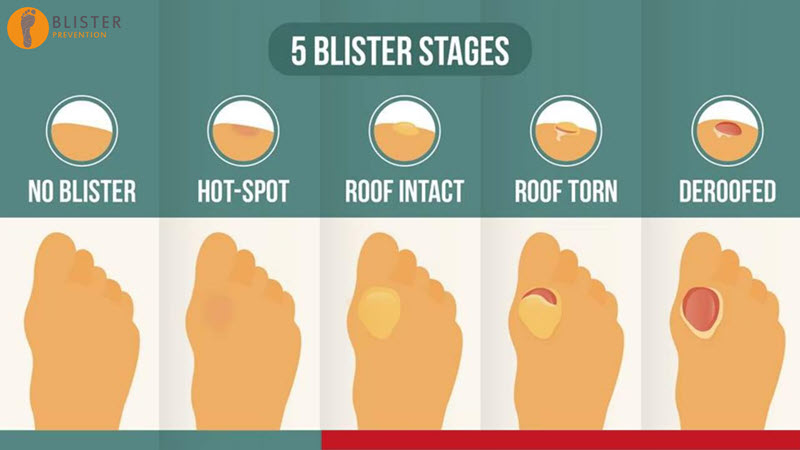
There are 5 blister stages. First there’s the blister-free stage, The idea is to stay here. Next there’s the hotspot stage. This is brief and usually either ignored or missed by the patient. Ideally, the stop and implement the prevention they had planned for this blister site. If we don’t do enough to stop the blister-causing forces, we end up with a blister with an intact roof. Then, if we still don’t do enough to stop the blister-causing forces, we end up with a torn blister. When we lance a blister, this is the stage we take it to – we turn an intact blister into a torn blister. Lastly, if we still don’t do enough to stop the blister-causing forces, we end up with a deroofed blister.
Let’s have a look at the pros and cons of each of the 3 blister stages: intact, torn and deroofed. Because there are nuances to the right treatment and I hope to go through those in this presentation.
Should blisters be left intact?
Pros of intact blister roof:
It can’t get infected
No gear or expertise needed*
Cons of intact blister roof:
- Often worsen (gets bigger/ hurts more)**
- Often tears spontaneously**
- Still needs monitoring
* not to lance, but shear reduction still needed
**can be mitigated with excellent shear reduction
Should blisters be lanced?
Pros of lancing blister roof:
- Can reduce discomfort***
- Controlled environment
- Small opening compared to deroofing reduces risk
- Prevents solidified fluid from becoming an irritant
Cons of lancing blister roof:
- Opens up to infection
- Needs gear and expertise
- Needs ongoing monitoring and care
***still needs shear reduction
Should blisters be deroofed?
Pros of deroofing:
- If infected, antiseptic can get full access
- If soiled, can clear debris and clean better
- Won’t refill
Cons of deroofing:
- Increased risk of infection due to larger surface area
- Less innate protection (no roof)
- Needs gear and expertise
- Needs ongoing monitoring and care
What about high risk patients?
Should blisters be lanced or deroofed at all in people with diabetes or issues of immunocompromise? Intuitively, the priorities in treating high risk patients include maintaining skin integrity. So there’s a big case in just leaving that blister intact. But don’t just leave it intact and think I’ve done the best I can because it’s intact and it won’t get infected. There’s nothing to say that five minutes later it’s still going to be intact. So you need to offload it – you need to implement a really good shear-reduction strategy, even if you leave that blister intact. We’re hard-wired into just thinking pressure when we say offloading, but there are other things that you can and should do, or at least think about (we’re going to get to that a bit later).
Keeping it intact also takes infection out of the equation, at least at that immediate stage. You’ve still got to offload it though. Otherwise it will tear.
The self-care is a tricky one. So if you leave a blister intact, And you send your patient on their way, can they see their blister to reassess it? Are they going to need some follow-up, even though you’ve left that blister intact? So you could argue that even though you’ve done nothing with the blister in terms of the integrity of the blister roof skin, we still need some professional monitoring and possibly treatment.
Blister Treatment Examples
Let’s go through some examples together and decide whether the blister roof should be left intact, torn, or deroofed. I’ll provide some context, then I’ll tell you how I’d deal with it. Feel free to join in and say if you’d do anything differently.
What would you do with this one? Would you leave it intact? Would you answer it or would you roof it?
Example 1: Outside of little toe
Example 2: Inside of little toe
Example 3: Under toenail 3rd toe
Example 4: Medial forefoot edge blisters
Example 5: Under 2nd metatarsal head, tracking towards 1/2 interdigital space
- Resolved/resolving plantar 1st met head blisters
- Infected blister central forefoot
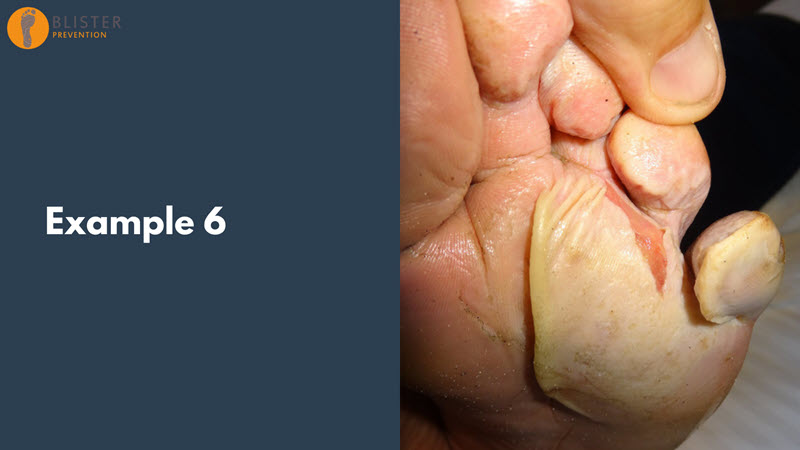
Example 6: Macerated torn blister under 4th and 5the metatarsal head
Example 7: Lateral heel edge blister
Example 8: Posterior heel
The tools I use
- Hand sanitiser & gloves
- Bluey
- Sterile cottonwool balls & buds
- Scalpel blade (no handle nec)
- Hypodermic needles (for toenail blisters)
- Sharps container
- Normal saline for irrigation
- Povidone iodine prep pad
- Sterile dressings
Alternative tools and methods
- Sewing needle
- Scissors/pocket knife
- +/- Sterilising with
- Flame or hand sanitiser
- Blister threading
- Hypodermic needle & syringe
- +/- Hotshot (Friar’s balsam)
- Nail trephination
- hot paperclip, nail drill or electrocautery pen
Q & A
Q1: To lance, deroof or leave – is it different for diabetes etc
Please watch the video for a full explanation.
Q2: Are there certain types of foot blisters that you believe should always be deroofed or lanced? How do you communicate these recommendations to your patients?
Please watch the video for a full explanation. However, my broad considerations are:
Deroof:
- Infected or soiled
- Hydrocolloid
- Non-viable roof skin
Lance:
- Likely to spontaneously tear
- Taut, thin skin, tracking
- Mid-activity, clean
- Gear
- Good self-care, able to access care
Leave intact:
- Patient preference
- Unable to self-care/access care
- Not impacted by wb or footwear
- Excellent shear reduction in place
- High risk, immunocompromise
Q3: Best treatment?
Please watch the video for a full explanation.
Q4: How to care for blisters during an extended athletic event (ie running from Lands End to John O’Groats on mixture of trails & roads?
Please watch the video for a full explanation.
Q5: How to manage ‘hot spots’
Please watch the video for a full explanation.